Dominique-Francois Gazielly M.D
Specialist in Orthopaedic Surgery
Associate-Professor of Tia Tong Shanghai University

3. Request specific imaging
MRI or Arthro-MRI is not systematic. Indeed, plain radiographs often provide sufficient information to make an accurate diagnosis. In our experience, ultrasonography is rarely requested. We prefer imaging on paper rather than on a CD, as sometimes it is impossible to read by computer software.
I. The patient consults for pain that interferes in the daily activities and prevents sleeping on the side
The pain is located on the lateral side of the arm: it is probably a lesion of the tendons of the rotator cuff. They can extend to the neck and chest and it may be a calcification of the shoulder. They can be associated with pain localized to the anterior side of the arm, there is an inflammation or injury with the long biceps tendon.
In all cases, we request radiography of the shoulder, an antero-posterior view in neutral rotation and an outlet view.
- Radiography in neutral rotation objectives a calcification of the shoulder. Accurate diagnosis of the cause of pain is done. Further imaging (MRI, ultrasonography) is not necessary.

- Radiography profile objectives an aggressive anterior acromial spur which can cause damage to the rotator cuff and biceps tendon. In this particulary case, the Arthro-MRI (MRI with injection of contrast liquid) is necessary since this specific examination will demonstrate the status of the rotator cuff tendons, a simple wear caused by the acromial bone spur or real tendon rupture. Arthro-MRI is more accurate than MRI. If the patient is claustrophobic, Arthro-CT Scan can replace the Arthro-MRI.

Pain on the acromioclavicular joint
- Imaging is necessary to establish an accurate diagnosis when there is no deformation after a fall. A radiography of the two side shoulders comparative may detect a lesion on the affected side of the outer part of the clavicle.
Pain is localized in the shoulder and associated with crunches
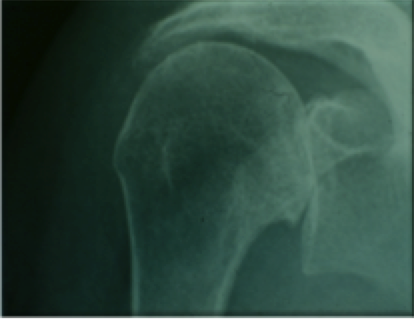
- Osteoarthritis of the shoulder is suspected clinically. In all cases, we request a radiograph in neutral rotation and the incidence of axillary profile.
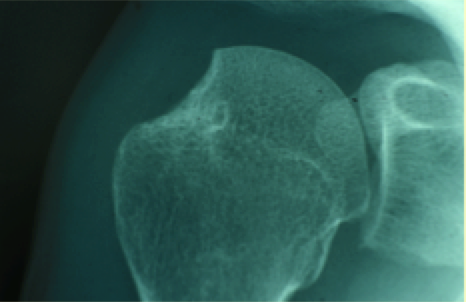
- The radiography in neutral rotation objective a Primary Osteoarthritis. Axillary profile provides information on the glenoid. A MRI will be necessary to confirm that the rotator cuff is retained, if the indication of total shoulder arthroplasty is considered for the patient.
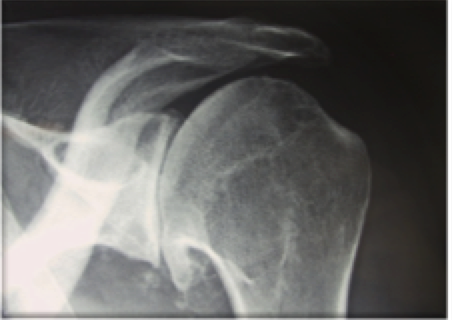
- The radiography in neutral rotation objectives an osteoarthritis with massive cuff tear, with a humeral head under the acromion ascended. We know from experience that the tendons of the rotator cuff are ruptured and irreparable, especially if the forward elevation is impossible with a complete loss of strength. MRI is not always necessary.
Pain leaves the neck to flow down the arms and accompanied by tingling in the hands.
- We send the patient to a rheumatologist or a spine surgeon, who will ask for the specific imaging to establish the correct diagnosis : plain radiographs and MRI of the cervical spine.
II. The patient consults because his shoulder was dislocated several times
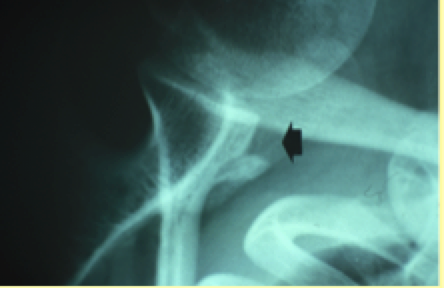
We request radiographs with two specific views which can make the diagnosis of anterior instability, showing bone lesions.
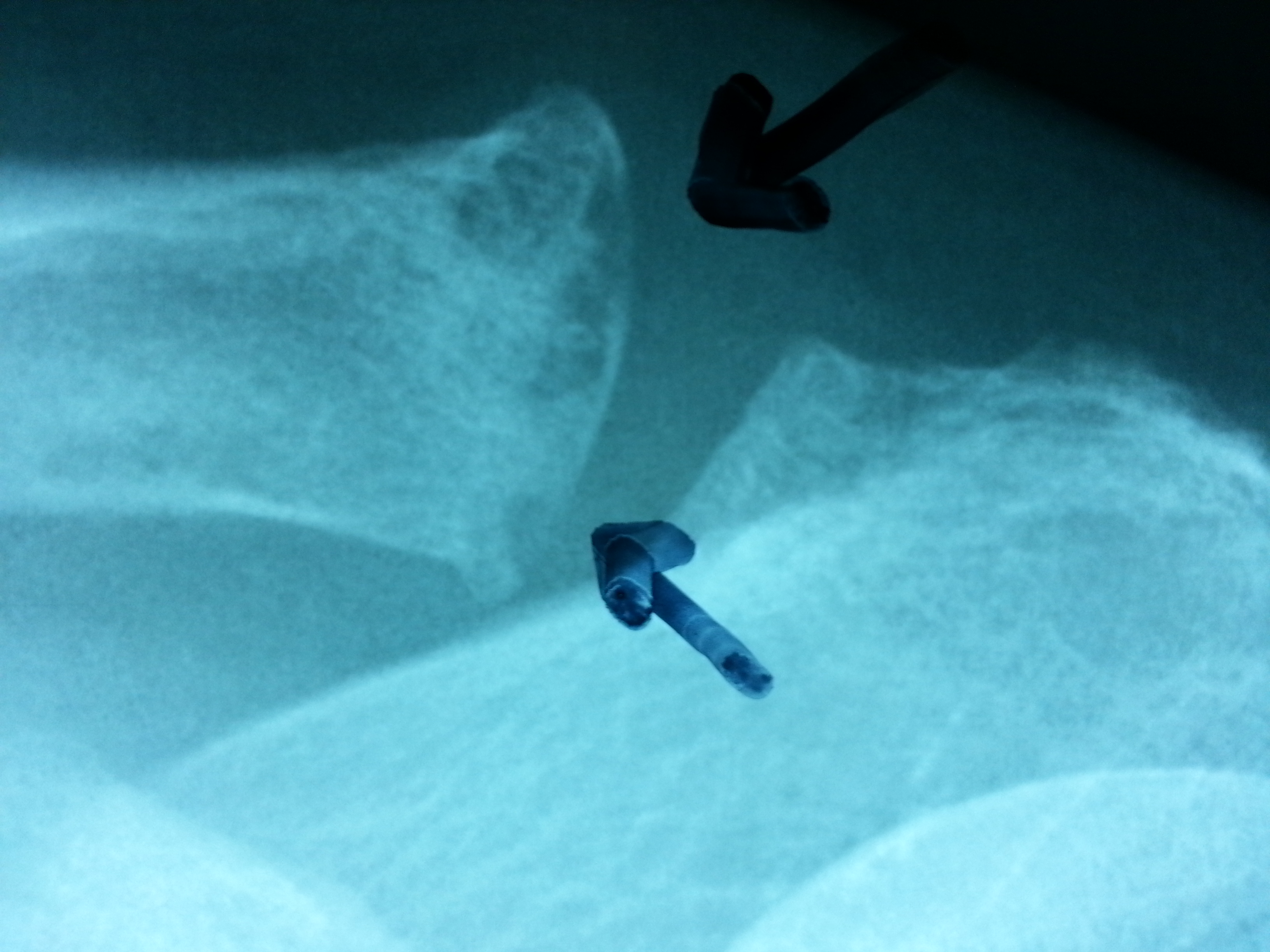
- Antero-posterior view in internal rotation can objectify a “notch” of the humeral head
- Bernageau view can objectify a fracture of the anterior glenoid’s rim. If plain radiographs show no bony injury, particularly if the subject is hyperlax. No other additional imaging is required (scanner, MRI).
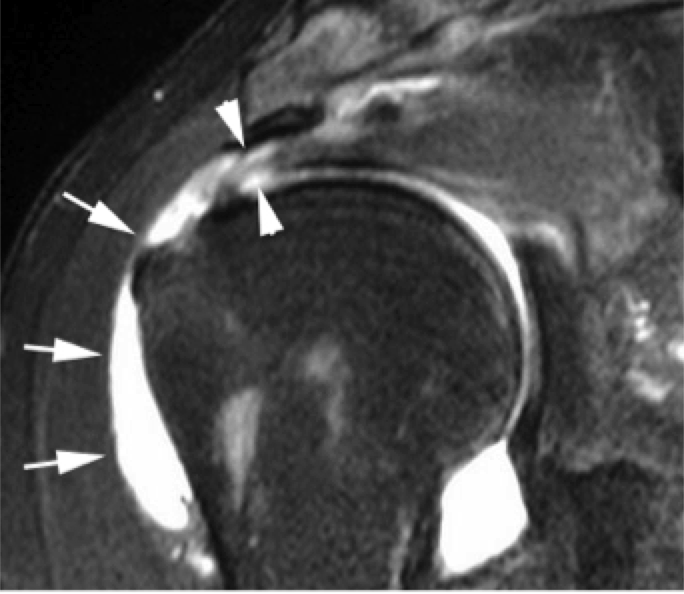
In this case, radiographs are requested to allow the diagnosis of anterior instability in objectifying a ligament Bankart lesion.
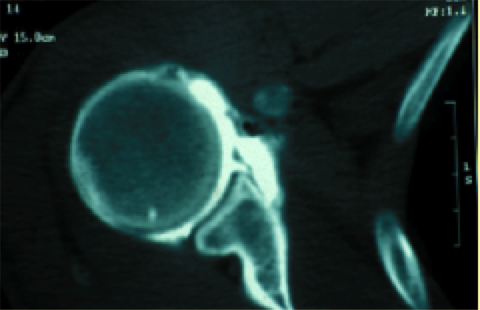
If the Arthro-CT Scan is normal, it will be necessary to perform an arthroscopic examination of the shoulder under general anaesthesia to establish an accurate diagnosis.