Dominique-Francois Gazielly M.D
Specialist in Orthopaedic Surgery
Associate-Professor of Tia Tong Shanghai University

2. Examine the patient
It is necessary to examine both shoulders, disrobed and cervical and thoracic spine.
The patient to be examined, just visit either for pain or because his shoulder dislocates.
I) The patient consults for pain.
The first question I ask the patient: "Show me where your pains are? "
o Pain on the side of the arm: it is probably a lesion of the tendons of the rotator cuff.
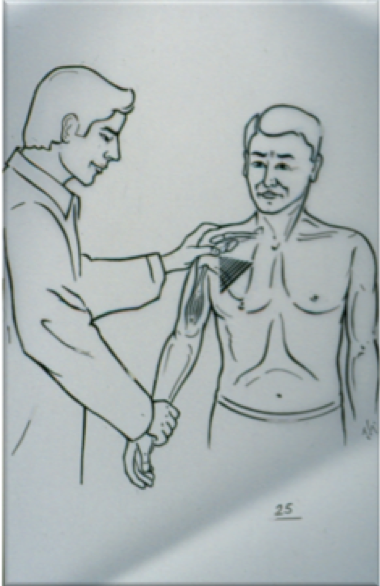
- I look immediately by a comparative examination of both shoulders, if there is a limitation of mobility of painful shoulder compared to the healthy shoulder.
- Limitation of mobility inforward elevation
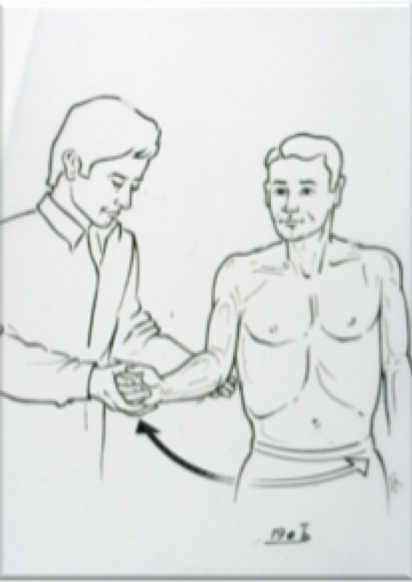
- Mobility limitationin external rotation
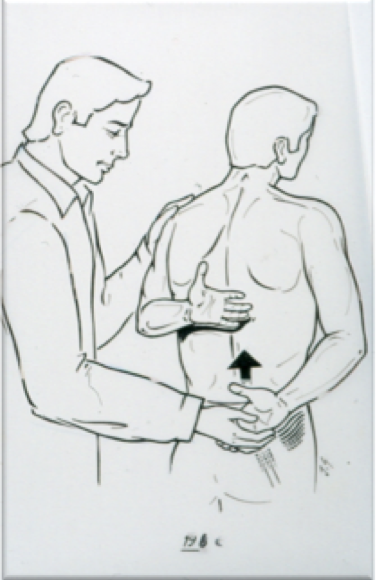
- Mobility limitationin internal rotation with a hand inthe back
- It is common that there is a certain degree of stiffness or a frozen shoulder, which amplifies the pain ... it creates a vicious cycle pain, stiffness, hence the importance of early diagnosis.
- Highly specific clinical tests can know during the clinical examination, if there is a rupture of one or more tendons of the rotator cuff caused by wear, friction and age, compounded by a possible fallon the shoulder. Imaging clarifies the diagnosis.
o Pain on the lateral side of the arm,extending to the neckand chest.
If the cardiac problem was eliminated, it is probably a calcification of the shoulder. Imaging clarifies the diagnosis.
o Pain on the front side of the arm
It is probably an inflammation of the long head of biceps, caused by repetitive movements(computer mouse, gardening, etc....)
o Pain on acronomio-clavicular joint
It may be the consequences of a simple fallor while playing sports(martial arts, ice hockey, rugby, skiing, horse riding, cycling), especially if there is anassociated strain. Imaging clarifies the diagnosis.

o Localized pain in the shoulder and associated with crunches every time the patient moves his arm.
- The arm mobility is reducedand painful. Most often,it is a patient over 65 years old, already wearing prosthesis of a hip or knee.
- Itis probably an OSTEOARTHRITIS of the shoulder
- If the patient can raise his arms above the horizontal, the tendons of the rotator cuff are probably preserved: this is called PRIMARY OSTEOARTHRITIS.
- If the patient is unable to elevate his arm up, the tendons of the rotator cuff have probably disappeared in an aged over 70patient: this is called an OSTEOARTHRITIS WITH MASSIVE CUFF TEAR.
- In both cases, the imaging clarifies the diagnosis.
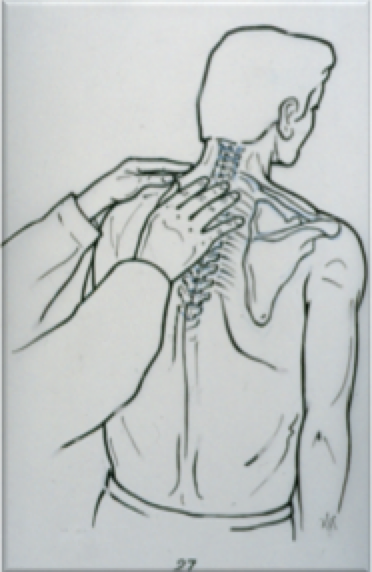
o Pain from the neck and down the arm to the fingers.
- The pain may be associated with naimless in the fingers.They are spontaneous orcaused by rotation or tilt of the neck: one speaks of cervico-brachial neuralgia, which can also be associated with lesions of the rotator cuff of the shoulder.This is why the examination of the cervical spine should be systematic.
- Imaging clarifies the diagnosis. (photo 8)
II) The patient consults because his shoulder was dislocated several times.
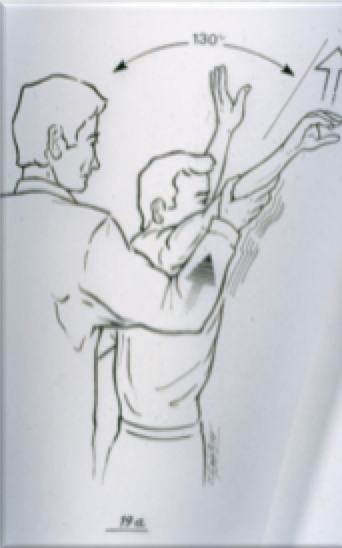
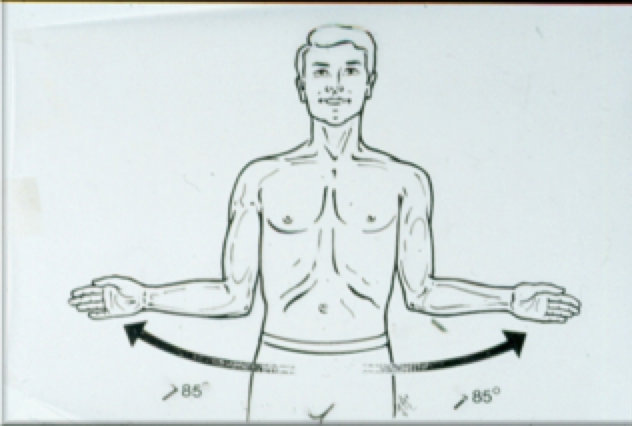
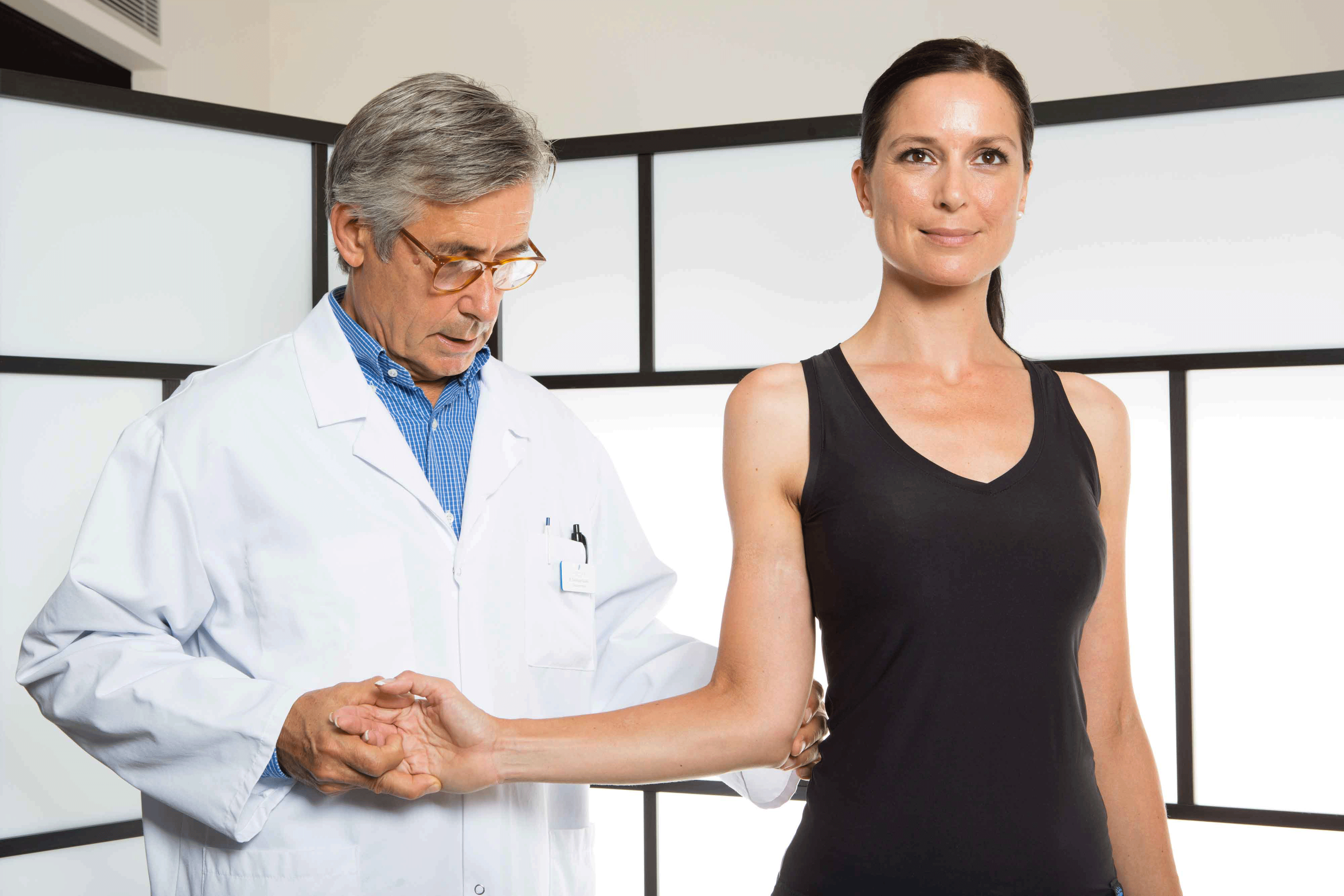
o The first thing I look at clinical examination is the existence of a constitutional hyperligamentous laxity: The patient's joints are too flexible, and we look for a history of recurrent sprains of the ankleorknee pain. This hyperligamentous laxity, resulting, at the shoulders, by excessive external rotation exceeding 85 degrees (Photo10). Hyperligamentous laxity aggravates shoulder instability.

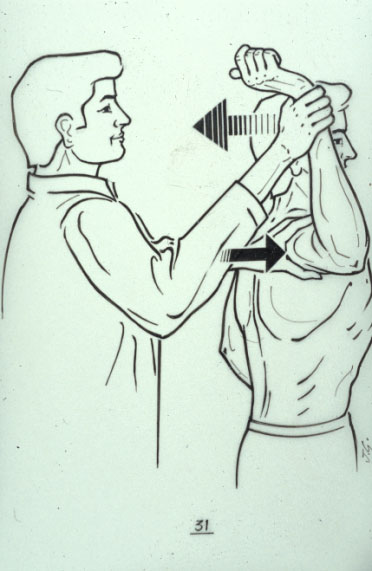
o Clinical examination research cautiously an apprehension of the patient, the shoulder is positioned in dislocation side, with an elevation process of the armabove the horizontal and it is associated with an external rotation (position of the handball shooting).
o Imaging clarifies the diagnosis.