Dominique-Francois Gazielly M.D
Specialist in Orthopaedic Surgery
Associate-Professor of Tia Tong Shanghai University

The Shoulder Surgery
1. Anesthesia and postoperative pain management.
o We carry all our shoulder surgeries, whatever the method, arthroscopic or “opened”, under general anesthesia. We do not associate a regional anesthesia by interscalenic block.

o Immediate postoperative pain is completely controlled by analgesics. A pump can be used for morphine for more than the average algic patients. But in our experience, this is the immediate post-operative passive mobilization, in a combination with cryotherapy (ice packs are applied on the shoulder), which is the best postoperative pain reliever.
o Patients operated by arthroscopic method, but not those performed by the "opened method", can, in theory, return home the evening of the day of surgery, after, they did with the physiotherapist, their first session of passive mobilization of the operated shoulder. This is what is called outpatient surgery. But in practice, we prefer to keep the patient in hospital overnight or even for 2 to 3 days, in case of an elderly patient, or living alone. Two sessions of passive mobilization of the operated shoulder, morning and evening, are then performed with the physiotherapist in our shoulder unit, associated with passive motion exercises that the patient is doing alone, four times a day (see the "rehabilitation chapter"). Ice packs are applied to the operated shoulder, between therapy sessions.
o Patients operated by the conventional surgery "opened method" remain hospitalized in our shoulder unit, on average, four days after surgery of the instability for an athlete, and 7 days after implantation of total shoulder prosthesis. As after arthroscopic shoulder surgery, passive mobilization of the operated shoulder starts from the day of surgery with a physiotherapist, and continued two times a day with the physiotherapist, and 4 times a day by the patient alone for the duration of the hospitalization (see the "reeducation chapter"). Applying an ice pack on his shoulder, operated by the "opened method" is even more necessary after arthroscopic surgery to relieve post-operative pain, which is, in any case moderate, the day after intervention.
2. Both methods of shoulder surgery.
The surgical procedure can be made either through small skin incisions 2 to 5 mm with a control, on a television monitor, of the image provided by a micro camera introduced inside the shoulder (arthroscopic surgery), or by skin incision a few inches, and an opening in the muscle wall (opened surgery).
We perform arthroscopic shoulder surgery, learned during our stays in the USA since the 1990s ...
- A revolutionary principle in the late 1980s, is to achieve a very precise technical surgery inside shoulder, under the control of an image, provided by a micro-camera inserted into shoulder, and sent on a television screen in front of the surgeon.
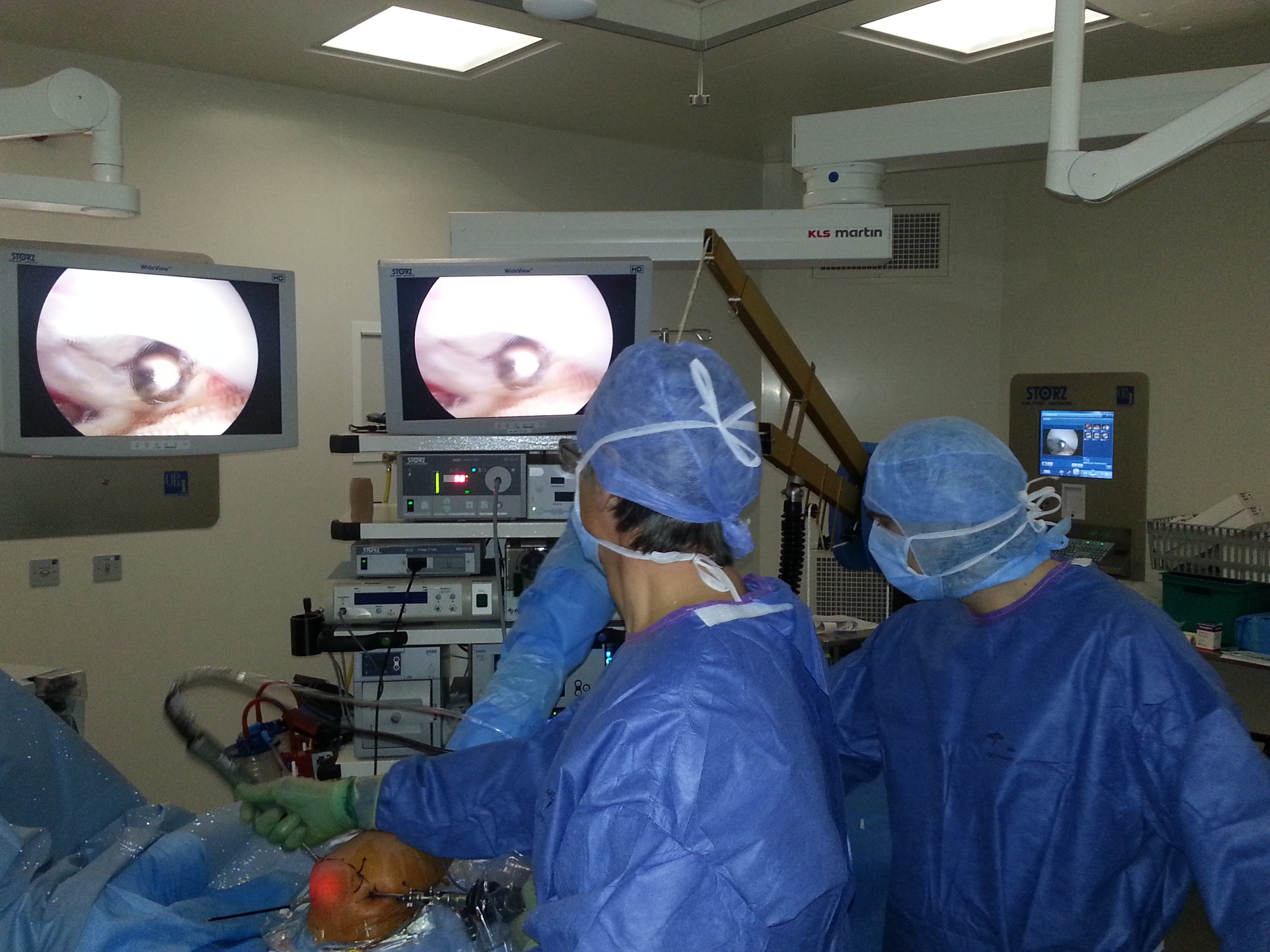
- A pump allows to get in and out, permanently, with a sterile saline solution, the surgeon can adjust the pressure and flow of the solution for an excellent visibility of tissue inside the shoulder. Specific surgical instruments, whose size does not exceed 4 mm, are used for this arthroscopic microsurgery.
- The advantages of arthroscopic shoulder microsurgery are recognized:
- There is, theoretically, no risk of an infection, because the inlet and the outlet, continuously cleaned by the sterile saline solution, prevent by a continuous washing of the shoulder, the ingress of any microbe.
- Postoperative pain is low, due to the absence of opening of the shoulder muscles.
- Cosmetic Benefits: Scars of 3-4 small skin micro-incisions are virtually invisible.
- We carry 80% of our surgeries by arthroscopic method:
- Removal of calcification deposit of the rotator cuff
- Removal of an aggressive acromial spur
- Repair of a ruptured rotator cuff
- Debridement of massive and irreparable rupture of the rotator cuff with tenotomy of a very degenerative long head of biceps
- Repair of a ligament for an athlete with a Bankart lesion
o We have operated all our patients by the opened method surgery from 1986 to 1992, before arthroscopic shoulder microsurgery becomes reliable and reproducible. The “opened" shoulder surgery still represents about 20% of our surgical practice.
- The post-operative infection risk is never absent. The objectives of the surgical team in the operating room or the care team in the shoulder unit, and overall for a care facility is to reduce the risk to zero. Be aware that the risk of postoperative infection is increased for some patients with a medical history: poorly controlled diabetes, urinary tract infections, poor dental hygiene, and skin acne.
- The immediate post-operative pain is now fully managed by a combination of effective therapeutics: anti-inflammatories and morphine pump are not systematic; analgesics, immediate postoperative passive mobilization and ice packs on the shoulder are systematics.
- The quality of the scar still holds our attention. But be aware that it is the patient who "makes" his scar ... for example, a patient with (too flexible joints) constitutional hyperlaxity can have a non cosmetic scar.
- We reserve today the "opened method " to three types of shoulder disorders:
- The majority of shoulder instability for athletes (previous anterior dislocations and subluxations).
We performed, with an “opened” procedure, what we call a triple locking of the shoulder (bony, muscular, ligamentous locking). The procedure can be called too “ Modified Bristow-Latarjet procedure”. This intervention, very carefully made, could return a direct sporting mobility, without any risk of subluxation or anterior dislocation.
- The centered primitive glenohumeral osteoarthritis requires the implantation of an “Anatomical Total Shoulder Arthroplasty”, which works in combination with the tendons of the rotator cuff, real "motor" of the prosthesis.
- The eccentric glenohumeral osteoarthritis with massive and irreparable rupture of the rotator cuff, requires the Implantation of a “Reversed Total Shoulder Arthroplasty”, which works with the deltoid muscle as a result of the disappearance of the rotator cuff.
Rehabilitation, postoperative recovery after each type of surgery, microsurgery performed arthroscopically or opened, are specified in the "reeducation chapter". Functional results after shoulder surgery are shown in the "Results chapter".